Contact dermatoscopy and polarised light
Knowledge of dermatoscopy for diagnostics
Around the world, dermatoscopy is used as a non-invasive screening method for skin cancer, since it significantly increases sensitivity and specificity compared to examinations performed with the naked eye.
Dermatoscopes can be used in contact or non-contact mode and with polarised or non-polarised light to make different skin structures visible for diagnosis.
There are essentially three dermatoscope-based examination modes:
- Non-polarised contact dermatoscopy
- Polarised contact dermatoscopy
- Polarised non-contact dermatoscopy
Switching between examination modes can prove helpful to practitioners in differential diagnostics.
Non-polarised contact dermatoscopy
In non-polarised dermatoscopy, the instrument is placed directly on the skin for examination. A contact liquid is needed so that the light can penetrate the stratum corneum and deeper layers of the skin can be assessed too.
In the simplest case, a dermatoscope consists of a focus-adjustable magnifying lens, a form of illumination and a transparent contact plate. A contact plate (a glass plate) is used since a large part of the light that hits the skin is normally reflected, this significantly reduces the amount of reflected light.
If a (contact) liquid is also applied to the skin lesion to be examined, the stratum corneum appears quasi-transparent, enabling the assessment of additional skin layers. Looking through the magnifying lens allows practitioners to see details that are invisible to the naked eye.
- Use of a contact liquid is essential for non-polarised contact dermatoscopy. The contact plate is located on the instrument.
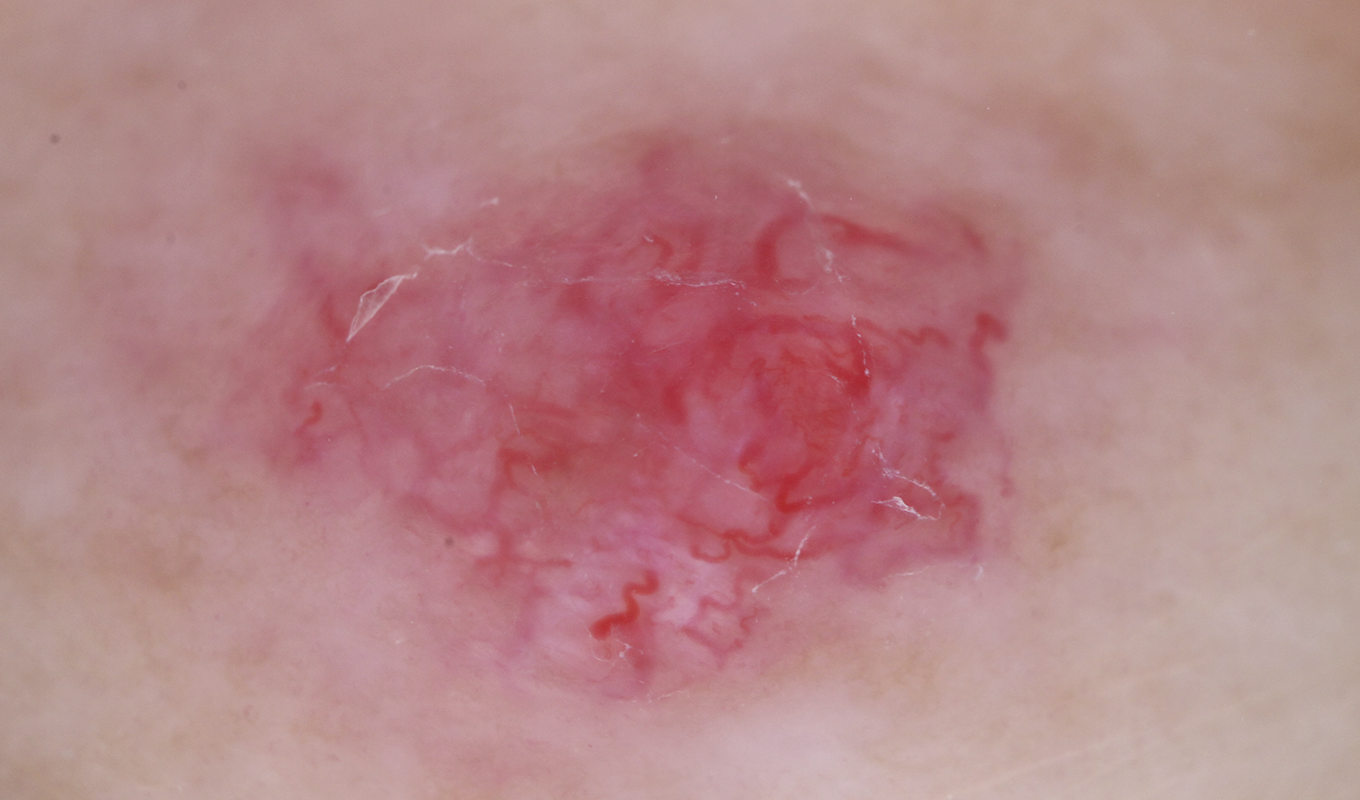
Image with non-polarised light
Disinfectant, immersion oil or ultrasound gel, for example, can be used as the contact liquid depending on the product specification.
- The benefits of using disinfectants include the simultaneous microbiocidal effect and the quick handling. However, it should be noted with some dermatoscopes the disinfectant should not be sprayed directly onto the contact plate; it should only be applied to the patient’s skin.
- Applying immersion oil provides very clear and distinct imaging due to the oil’s viscosity.
- Ultrasound gel offers benefits when it comes to assessing vascular structures, since next to no pressure needs to be applied on the skin here. The contact plate will glide on the gel. What’s more, the gel can even out any unevenness, like that encountered when examining the nail fold or the nail plate.
Once the examination is complete, the contact plate must always be wiped with a disinfectant cloth.
Some dermatoscopes come with a small contact plate too. This is beneficial because it enables assessment of hard-to-reach structures like the interdigital space. A non-contact, polarised dermatoscope (or an equivalent mode) can be used here as an alternative.
Polarised contact dermatoscopy
In polarised mode (polarised dermatoscopy), the light reflected on the surface of the skin is blocked out by a (polarisation) filter. Therefore, the visibility of deeper structures of the epidermis can be increased.
- The instrument rests on the skin with the contact plate in place. In polarised contact mode, use of a liquid is not mandatory.
Contact dermatoscopy – whether non-polarised or polarised – involves applying pressure to the area of the skin to be examined. On the one hand, this can lead to a distorted representation of the examined areas’ skin geometry. On the other, circulation is also reduced at certain points, making small vascular structures more difficult to detect, for instance in case of basal cell carcinoma. Therefore, non-contact dermatoscopy is used as an additional examination mode:
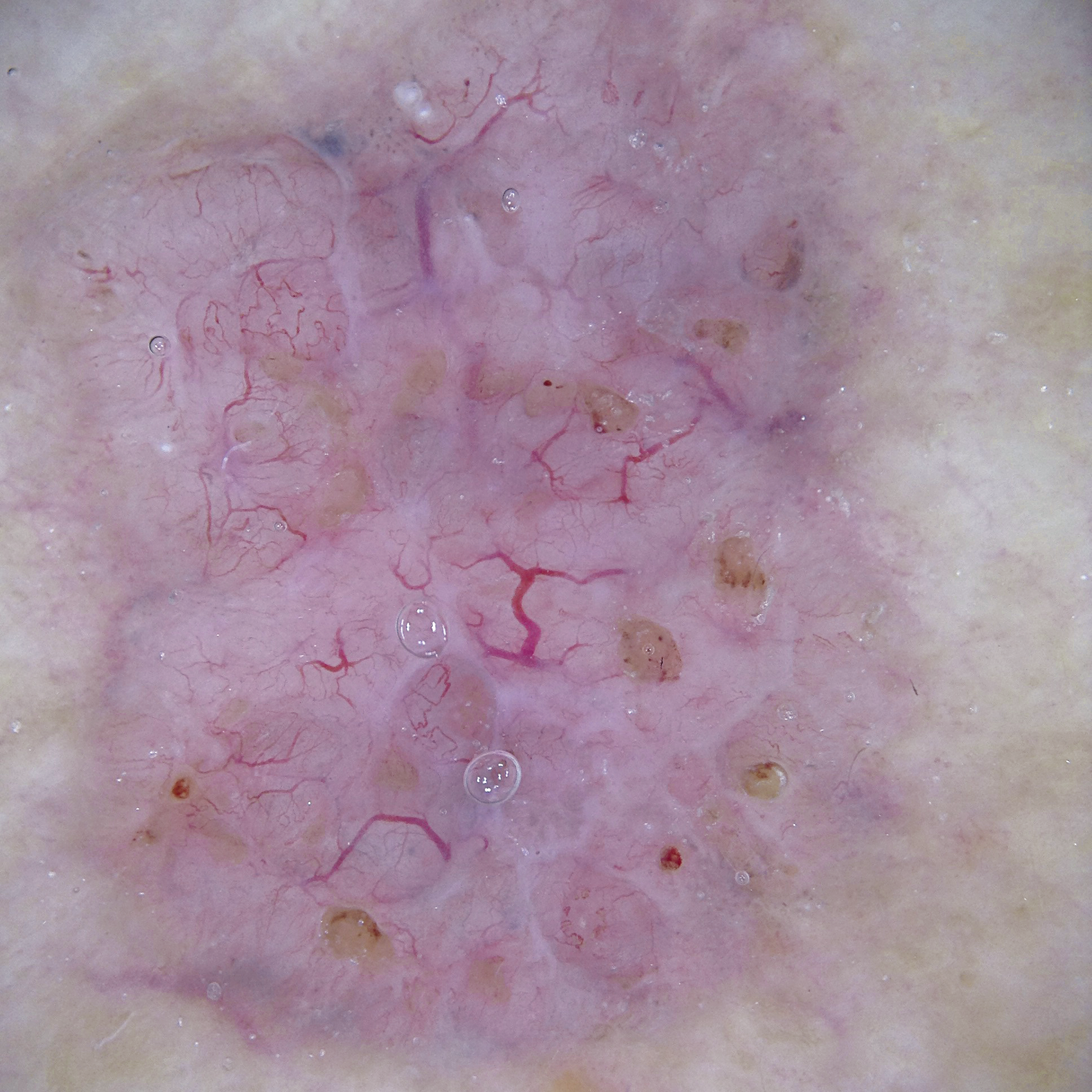
Image with non-polarised light
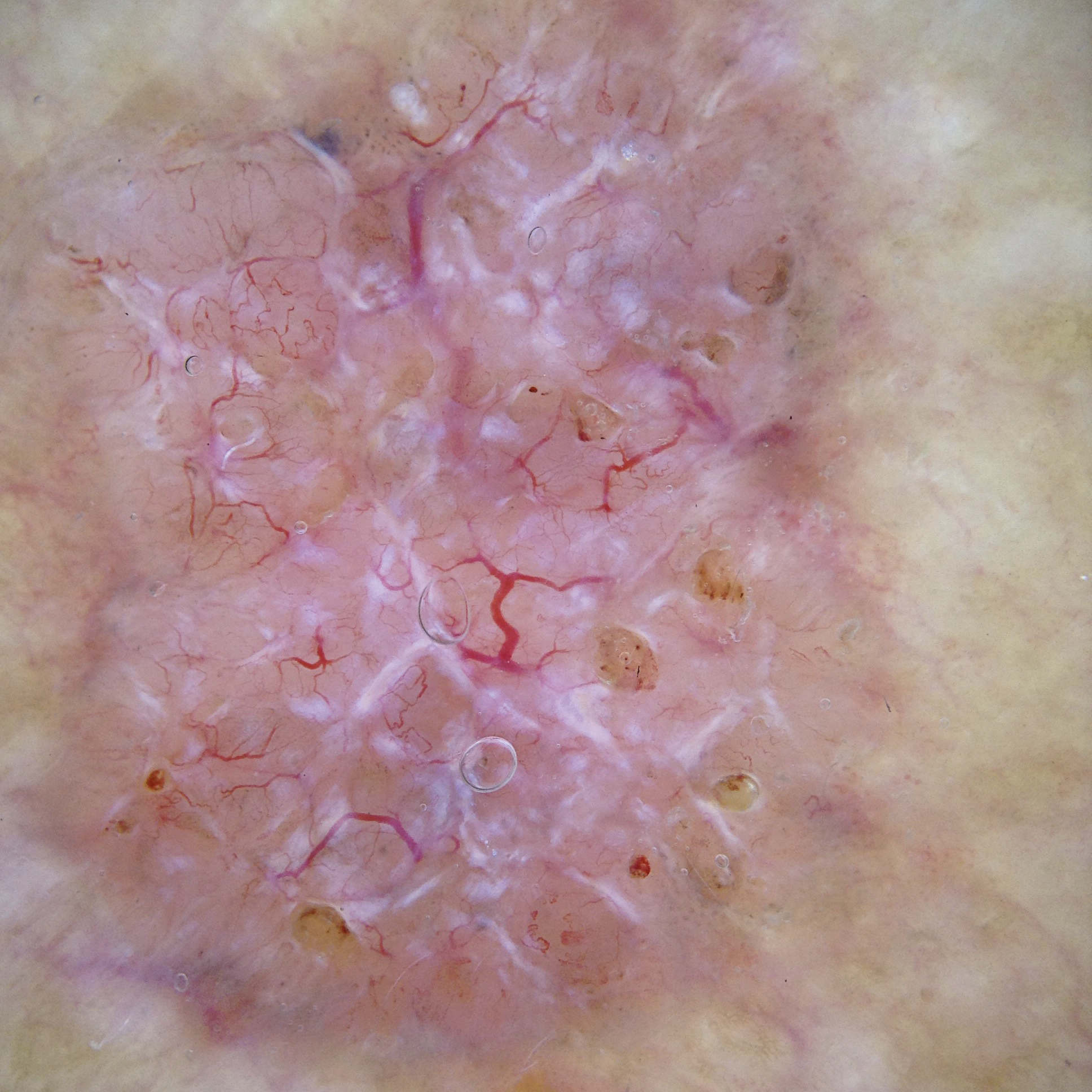
Image with polarised light
Polarised non-contact dermatoscopy
Polarised illumination permits performance of dermatoscopy examinations in non-contact mode too. The dermatoscope’s contact plate is removed for this purpose, and areas of the skin can be examined from a short distance.
Additionally, this mode is particularly suitable for examining infected areas and lesions that are painful for the patient because the non-contact examination means that no pressure is exerted on the areas of skin to be examined.
- The instrument’s contact plate is removed for this examination mode. Use of a contact liquid is not necessary here.
- Alternatively, the diSTANCE working ring can be used instead of the contact plate. It enables pressure-free examination of raised skin lesions and superficial vessels, maintaining a constant distance between the skin and the dermatoscope.
Switching from polarised to non-polarised light
Switching between polarised and non-polarised illumination helps with differentiated assessment and diagnosis. For example, when using the HEINE DELTA 30 PRO, DELTA 30 or DELTAone, it is easy to switch from one mode to the other (toggle button). There is no need to change the contact plate. Polarisation illumination is automatically available when the instrument is switched on.
Example: Melanoma

Image with non-polarised light
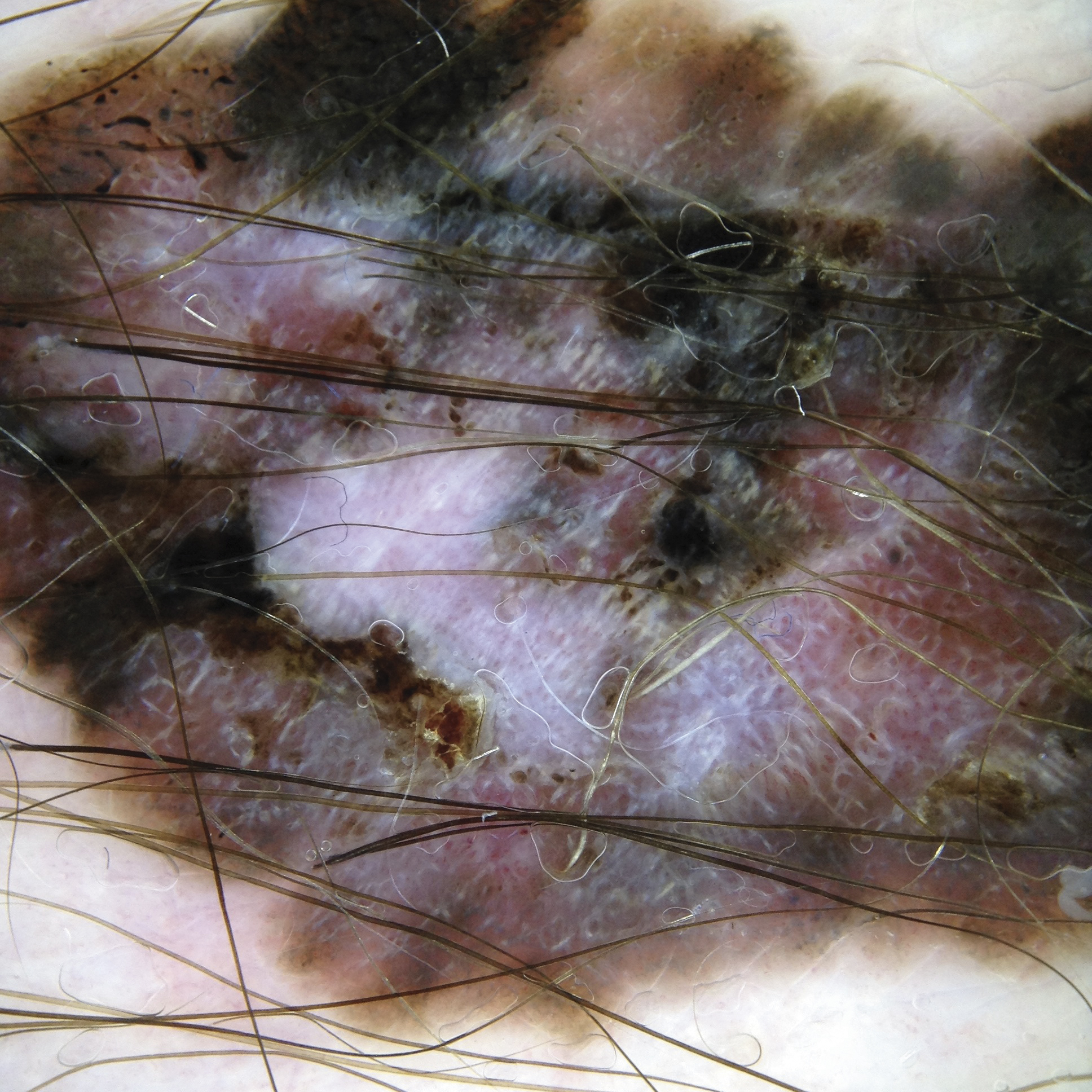
Image with polarised light
Differential diagnostics with polarised and non-polarised light
Modern dermatoscopes allow practitioners to switch between polarised and non-polarised light modes. The two types of illumination visualise different skin structures and therefore provide the practitioner with additional information – depending on the issue.
Subject to the position in the skin, some structures can be better identified with polarisation, while others are easier recognised without polarisation.
Which structures of the skin can be better visualised with non-polarised or polarised dermatoscopy in contact mode?
| Non-polarised contact dermatoscopy | Polarised contact dermatoscopy |
|---|---|
| Superficial structures (superficial epidermis to the dermoepidermal junction zone). | Deeper structures (e.g. at the level of the dermoepidermal junction (DEJ) or the upper dermis). |
| Superficial whitish structures of an orthokeratosis. | Crystalline structures and rosette-shaped structures in the skin lesions as what are known as ‘shiny white structures’, which are associated with more collagen and are thus localised deeper. This is frequently the case when diagnosing basal cell carcinomas. |
| Blue-white structures in a malignant melanoma’s regression zone. | In pigmented lesions with melanin at the dermoepidermal junction zone or in the dermis (junctional or blue naevi), somewhat darker shades of black and brown tones and occasionally greater variability in the pigment pattern are often observed here. |
Horn pseudocysts or pseudo-follicular cavities in seborrheic keratosis. | Vascular patterns and vascular redness (since the vessels lie in the dermis and can be examined without any pressure effect). |





