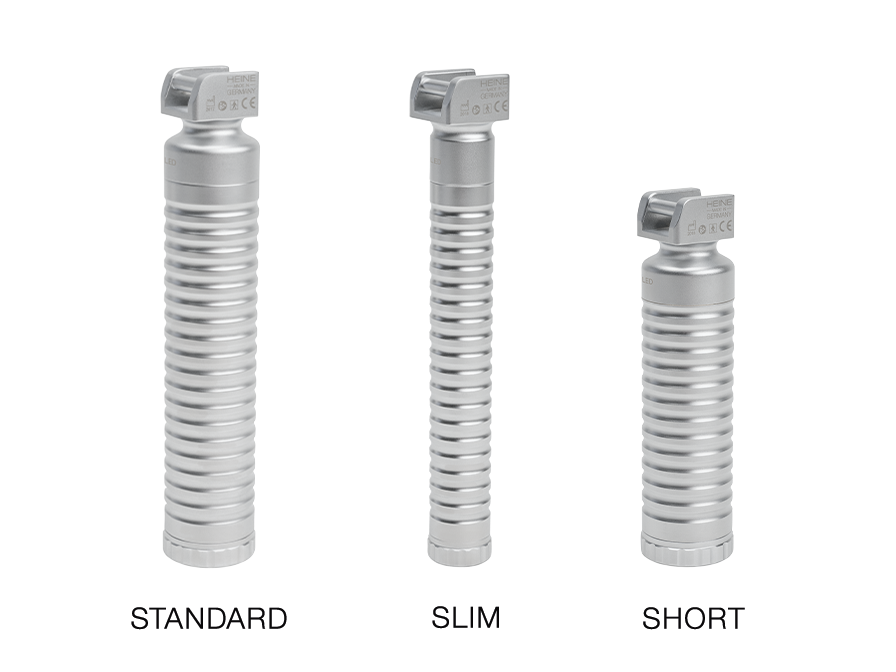
Three laryngoscope handles for different intubation situations
Standard, slim or short
While oral intubation is essential for securing the airways, it is very challenging in terms of technique. It poses major challenges for examiners and the entire team. In this regard, a high intubation success rate plays a directly crucial role in improving outcomes in critically ill patients. This is true of both oral and nasal intubation.
It is why the right technique, regular training and the expertise acquired with intubation all play a major role. But it also depends on choosing the right instruments, because they can provide strong support in successfully intubating patients in difficult situations.
Both the choice of the various blade types and the different shapes of laryngoscope handle have an influence on how easily, quickly and complication-free intubation is to perform.
The following tips relating to using different handle shapes (slim, short and standard) are intended to give practitioners a rough guide as to which handles are most suitable in which situations.
Thin, long laryngoscope handle (slim)
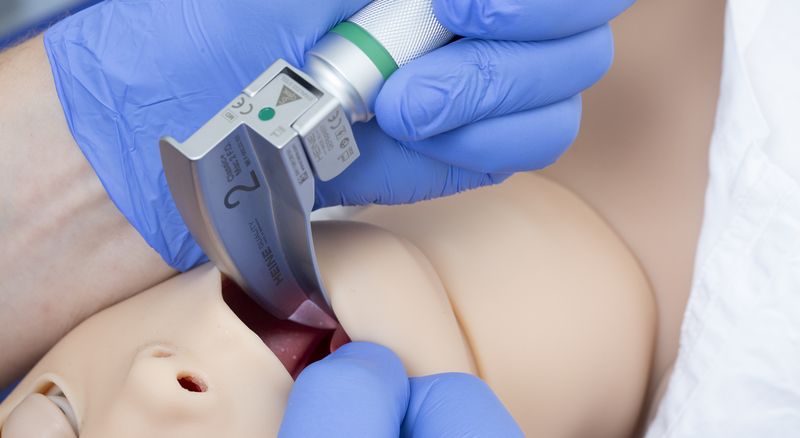
The slim handle is well suited to intubation where space is tight due to the thorax being prominent, the back of the head being large and prominent and the neck being short, as is the case with the delicate airway in paediatric patients.
Tip N°1: Particularly fine motor work possible
During normal adult intubation, the examiner usually holds a standard handle with their entire left hand so they can perform the necessary technique by pulling ventrally. But when dealing with children, practitioners require more fine motor skills and the available space is significantly limited. It is important to avoid the need to adjust or ‘lever’ the laryngoscope due to the cramped conditions.
The slim, lightweight shape allows the examiner to grip this handle with 2 or 3 fingers and guide it very well during use. The examiner retains the necessary fine control of the laryngoscope when it comes to correcting positions.

Tip N°2: Light weight means it sits snugly in the hand
The slim laryngoscope handle weighs far less than the standard model. The light weight has a positive impact on the paediatric respiratory tract because it can reduce the local complications and secondary damage caused more quickly.
Tip N°3: More application-related scope
When intubating paediatric patients, the head is positioned differently compared to the one used when intubating adults. The routinely preferred position is the sniffing position (neutral position). But, in this position, there is less room for the laryngoscope handle compared to the child’s thorax, meaning the handle might bump against the thorax when it is inserted into the oral cavity.
The circumference of the slim handle is about a third smaller than the standard handle, enabling more flexible handling.
Tip N°4: Ergonomic handling for examiners with small, slender hands
But the slim handle isn’t just particularly suitable for treating children. It also offers examiners with slender hands clear benefits when it comes to handling.
The reduced handle circumference means the slim handle fits better in small hands than the wider and heavier standard handle. It can also be used for intubating adults.
Thick, short laryngoscope handle (short)
Tip N°1: More room to move where space is tight
The improved Jackson’s position is usually used for adults. However, despite the head being in a higher and hyperextended position, it may be difficult to insert the laryngoscope in certain patients with a prominent thorax. The handle might bump into anatomically exposed areas, limiting flexibility in guiding the laryngoscope.
The short handle can show off its strengths with this group of patients. The short shape permits easier positioning, even if the patient has a prominent thorax.
At the same time, the handle’s wide cross-section maintains the feeling for good control.
Tip N°2: Compact handle for mobile applications where every gram counts
With its compact design, the short laryngoscope handle combines the standard handle’s basic features with space and weight savings. This pays off, especially in mobile applications where life-saving equipment needs to be lightweight, handy and compact (in the likes of internal hospital emergency teams, in rescue services or in special applications such as mountain rescue).

Laryngoscope standard handle (standard)
The globally established standard handle has proven its worth in its existing shape in use for classic intubation.
Tip N°1: Longer battery life for more intubations
The standard handle has room for more and larger batteries making the battery last up to twice as long. So the regular laryngoscope handle proves to be particularly reliable in everyday continuous use.
Tip N°2: Helpers for handling support
In certain situations, an increased amount of force may be required to adjust the visual axis to the vocal cords. This must then also be maintained until the endotracheal tube is successfully placed in the trachea.
It can be helpful if a helper holds the upper end of the handle as instructed by the intubator and provides specific support when guiding or pulling the laryngoscope.

Suitable handle variants for different intubation situations
Since different handles can make intubation easier depending on the situation, it makes sense to keep different handles in stock – if possible.
The above tips can and should only be suggestions that we have compiled by exchanging ideas with anaesthetists. They are not direct recommendations. Appropriate instruments are always and exclusively chosen at the trained examiner’s discretion.
What is the procedure for oral endotracheal intubation?
In technical terms, intubation by direct laryngoscopy involves inserting the blade into the oral cavity.
A standardised and well-established technique when using curved blades is to insert the laryngoscope into the right corner of the patient’s mouth.
Turning the laryngoscope handle medially should now cause the tongue to be moved by the blade. This rotation can be made more difficult by patient-specific and/or positioning-related factors, not to mention measures that need to be implemented in parallel.
You must be able to see the valeculla and glottis, plus the vocal cords and arytenoid cartilage, afterwards. Choosing the right shape of blade to use and a suitable handle (slim, short or standard handle) can be helpful depending on the patient and the situation.
More information
Laryngoscope blade options for intubating paediatric patients.

There are 27 good reasons to trust the quality of HEINE blades.

HEINE Blades are worth their price.

Laryngoscope Blades and Handles