White and black skin Cancer
Carcinoma
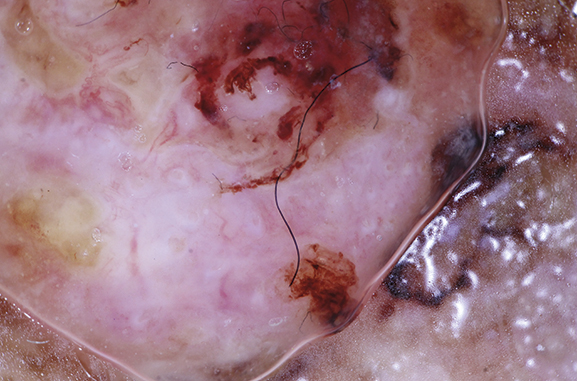
Basal cell carcinoma
Basal cell carcinoma typically occurs in elderly men; however, women and younger individuals can also be affected. The typical localisation is the bridge of the nose and other areas of the face. One particular form, superficial basal cell carcinoma, is often found on the torso.
Basal cell carcinoma spreads slowly and is infiltrative and destructive. It involves skin-coloured, shiny nodes that are frequently surrounded by dilated vessels (telangiectasia) and nodules arranged like strings of pearls. There is also a depression in the centre, which can also bleed.
Basal cell carcinomas are destructive but do not metastasise. They can therefore not cause metastases in other organs. Basal cell carcinoma is usually treated with surgical removal. Because basal cell carcinoma often forms invisible strands of tumours, the histological preparation should be examined for residual tumours along all the edges (3D histology). In some cases, follow-up surgery is required. Several surgical steps are often planned from the beginning.

Basal cell carcinoma
Squamous cell carcinoma
Squamous cell carcinoma also tends to affect the elderly. It primarily affects the face and results from many years of exposure to sunlight. Other affected areas include the outer ears, the lower eyelids, the bridge of the nose and the lower lip. Squamous cell carcinoma often develops from actinic keratosis, also known as sun warts. These are flat, reddish, and slightly scaling changes that cause slight discomfort. Occasionally, sensitivity to the touch or mild itching is reported.
In the transition to squamous cell carcinoma, an increased horn formation, a nodular growth, and a bleeding disorder may develop. The treatment of choice is surgical removal, followed by the histological examination of all edges (3D histology). If the histological examination reveals a particularly aggressive growth, or if the tumour exceeds a certain thickness (penetration depth), a sentinel lymph node biopsy is recommended for squamous cell carcinoma, as is the case for melanoma. In this way, a possible metastasis of tumour cells in the associated lymph nodes stations can be detected.
Unlike basal cell carcinoma, in squamous cell carcinoma, malignant cells can metastasise in the associated lymph nodes (and remote organs in rare cases). However, in most cases, this type of skin cancer can be detected and treated with surgery.
Squamous cell carcinoma
Melanoma
Malignant melanoma arises from the pigment cells of the skin. The colour is usually black, but there are also bright variants (amelanotic melanomas), which are particularly difficult to detect.
Most melanomas develop on the trunk and extremities, sometimes from pre-existing moles and sometimes from new ones. Other sites include the face (especially in the elderly), nails, the soles of the feet, mucous membranes, and the eyes (uveal melanoma). Men and women are equally affected, often between the ages of 50 and 60. However, malignant melanoma also occurs in young people.
The danger of malignant melanoma increases with tumour thickness: in the case of thin melanomas (< 1 mm), the risk of metastasis later on is low; in the case of thick melanomas (> 4 mm), there is a higher risk. Fortunately, thin melanomas can be detected early and removed with a safety margin.
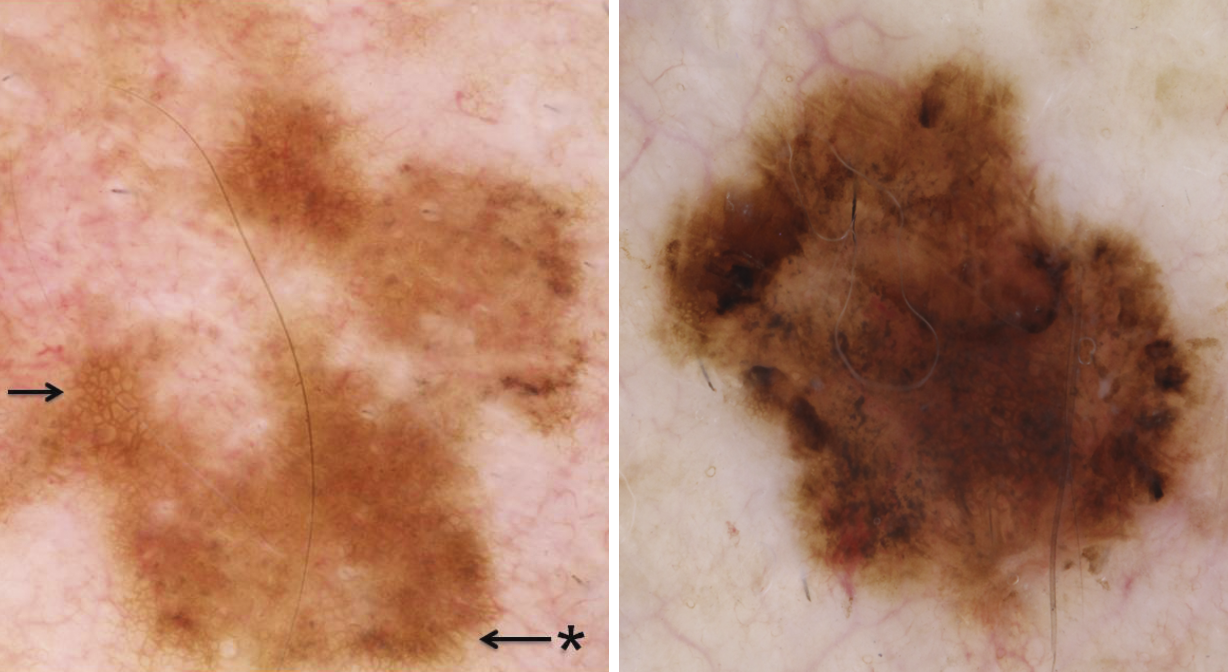
Melanoma in-situ